“[…] The midbrain doesn’t know the difference between a hit of cocaine and the ‘win’ of a social spotlight or a piece of band merch. It simply flags the object as a vital resource.
“When that happens, the brain’s priority-sorting software gets a bug. It starts assigning a ‘survival score’ to the pursuit that is higher than the score for food or family.
“The defining feature of this state is the persistent seeking of the object and a stark, undeniable inability to stop…”
The following Letter to the Editor on addiction was submitted to Wired868 by Dr Russell Lutchman, consultant forensic psychiatrist, Birmingham, UK:

(via iMind Mental Health Solutions.)
In my 35 years practicing psychiatry here in Britain, few scenes have cut deeper than watching individuals succumb to a lethal agent sold legally—that poisonous brew of nicotine and tar—all the while insisting they are merely enacting free will, embracing a personal choice.
But it is seldom about real choice.
Such minds labour tirelessly to construct elaborate fictions; fragile scaffolds of reason around their own ruin. These are minds hijacked, unknowingly to themselves.
What they call will is but an echo in an empty hall—the phantom of a freedom long since surrendered.
It isn’t just tobacco. Alcohol, cannabis, and other chemicals do their quiet work, trimming years off lives before a person even notices the shift. But we have to look past the chemistry to understand the full landscape of the hijack.
My experience has shown me that the journals and textbooks are often lagging behind. They focus on what they can measure in blood tests while missing the “invisible” addictions that dismantle lives just as thoroughly.
I use the term addictive pursuits to cover it all: the chemicals, yes, but also gambling, pornography, sex addiction, and what I call “spotlight” addiction—the persistent, ruinous craving for social gatherings and the intensity of being the centre of attention.

To make sense of these addictive pursuits, I use the biopsychosocial model. In practice, the “Bio” part usually gets all the attention because it feels scientific, while the “Social” and “Psychological” parts are treated like background noise.
From a biological standpoint, psychiatrists are looking at a brain whose survival hardware has been seized. Psychologically, we see the engine of self-deception—the “I can stop whenever I like” mantra. Socially, we see a world that provides “objects” that act like drugs.
Whether it is a cigarette or the roar of a crowd, the underlying mechanism is a unified seeking behaviour. If we ignore the non-chemical pursuits, we ignore more than half the problem.
This publication is for those ready to move towards the exit. Knowledge is power, but only when it is activated, focused and directed.
I first realised how narrow our clinical vision was in 1992. I met a young mother who presented with a depressed mood. As she spoke, however, the true nature of her crisis emerged: she was spending so excessively on merch supporting her favourite band that her child was left without enough to eat.
Her depression was the inevitable fallout of a life made impoverished by a compulsion she recognised, but was powerless to stop.
When I suggested to my seniors that this was an addiction, they frowned. They told me there were “loads of people like her” and that we didn’t need to be “medicalising” everyone.
So, they treated her depression—the symptom—and left the addictive engine untouched.

(via Vector.)
This case illustrates what I call a “survival error.” To the brain, there is no separate bin for “chemical” and “psychological” rewards. There is only a survival signal.
The midbrain doesn’t know the difference between a hit of cocaine and the “win” of a social spotlight or a piece of band merch. It simply flags the object as a vital resource.
When that happens, the brain’s priority-sorting software gets a bug. It starts assigning a “survival score” to the pursuit that is higher than the score for food or family.
The defining feature of this state is the persistent seeking of the object and a stark, undeniable inability to stop. It is important to distinguish this from recreational use.

(via Brandfoundry.com.au.)
Many people can use a substance or visit a casino and stop for weeks or months. But for others, the hijack is swift. With cocaine, the pathways can be seized in a single use. Tobacco may take longer, but the hook is usually set within a few weeks.
I use a three-year timeframe as a vital non-clinical metric for persistent addiction. By the time a pursuit has lasted three years, it has usually settled into the architecture of the mind as a permanent fixture. By then, “choice” has been outsourced to deeper, older parts of the brain.
The scale of this is staggering. The World Health Organization’s 2025 Tobacco Trends Report indicates about 1.2 billion people are hooked on nicotine. The UNODC World Drug Report 2025 adds 64 million with drug disorders and approximately 200 million with alcohol dependence.

(via Shutterstock.)
Across the globe, over a billion people are living in a state where their logic is compromised by an artificial necessity.
The experiences of hunger and thirst represent fundamental biological drives rather than mere preferences. Similarly, addiction operates by co-opting these same neural pathways, resulting in a comparable subjective imperative.
Under such conditions, rational cognition is significantly compromised. Unlike a mild bodily cue, addiction manifests as an overpowering demand that can appear as essential to the individual as sustenance itself.
In the face of such a primal, survival-like drive, logical reasoning often proves ineffective.

The “need” an addict feels for their pursuit—whether it is a drink or the spotlight of a party—mimics the primal urgency of starvation. Once these pathways are engaged, the “cognitive estate” is dominated.
Established routines, responsibilities, and even relationships are neglected as the drive for the “need” takes precedence. Even avoidance of articles like this one is often a defensive move orchestrated by those deep-seated pathways to maintain the hijack.
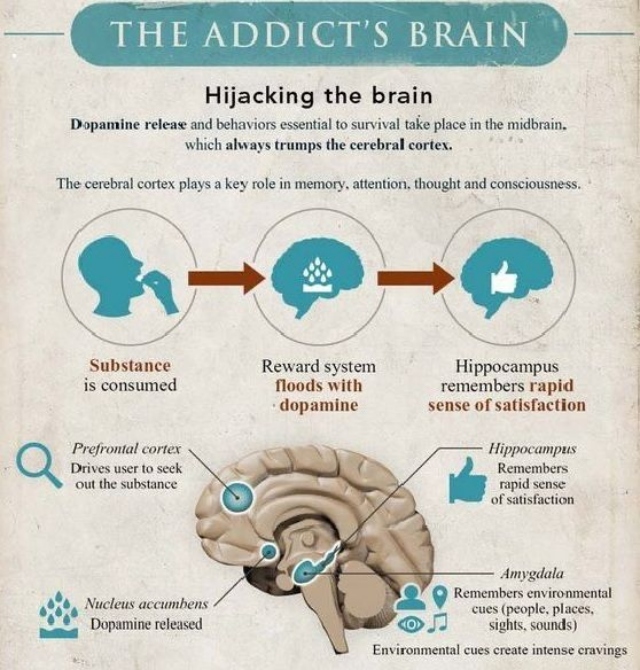
When addictive pursuits are engaged over years, they rewrite the mesolimbic dopamine pathway: the brain’s reward circuit. This circuit originates in the ventral tegmental area (VTA) and projects to the nucleus accumbens (NAc).
Addictive objects cause a surge of dopamine that far exceeds natural rewards.

This is where the chemical and the behavioural unify. The “near miss” in gambling or the anticipation of a social gathering activates the same dopamine surge as cocaine. Other regions are quickly embroiled:
- The Prefrontal Cortex: Responsible for judgement and impulse control, it becomes impaired. This is why the person can’t “just stop”.
- The Amygdala: Becomes hyper-responsive to cues and withdrawal, driving the negative emotional states that perpetuate the cycle.
- The Hippocampus: Vital for memory, it links environmental cues with the reward, triggering intense cravings whenever those triggers are encountered.
One of the greatest hurdles to recovery is what looks like self-deception. It is important to realise that this isn’t a case of someone simply “fooling themselves” in a casual way. Rather, the biological unwiring of the brain actually shapes the conscious narrative.

(via Rehab Today.)
In a healthy mind, the prefrontal cortex acts like a judge, weighing evidence and making rational decisions. In the hijacked mind, this region is co-opted—it becomes more like a defence lawyer, constructing brilliant arguments to justify the “need” the midbrain is screaming for.
The person is sincere in their belief that they are in control because their very capacity for self-observation is being fed corrupted data. This resemblance to anosognosia—the failure to recognise a health problem—is a direct result of the brain’s decision-making architecture being rewired to protect the pursuit.
It is not just stubbornness; it is a mind ensnared by a twisted survival instinct.
In the UK and elsewhere, we often hear warnings against “medicalising” behaviour. This has become a political term used to gatekeep resources.

By refusing to “medicalise” a pursuit that has clearly hijacked the brain’s survival machinery, the patient is effectively abandoned. Secondary symptoms like depression take focus and are treated because they fit the books, while the primary engine of destruction is dismissed as a “lifestyle choice”.
Overcoming an addictive pursuit involves a significant recalibration of these hijacked pathways. It starts with recognising that the “need” isn’t a character flaw—it is a biological error.
Logic has been sidelined by a force that feels as fundamental as feeding. Understanding these mechanisms should not lead to despair, but to a place of informed compassion.

Whether the object is a substance or something less tangible, the path to recovery involves moving from denial into contemplation, supported by a system that is willing to manage the whole landscape of the hijack.

“[…] I remember July 27, 1990—the fear, the uncertainty, the families gathered around radios and television sets. The attempted coup Read more

“[…] (John Aboud’s Superior Hotels) consistently refused to adjust the project’s scale, design, or mitigation strategies, demonstrating a profound lack Read more

I was a fair way into my column when the call came. It was from one of the sharpest, most Read more

There is something quietly disarming about watching a child see a giraffe in the zoo for the first time. The Read more

A recent comment from a visiting sailor has stayed with me in a way that is both embarrassing and deeply Read more

“[…] In his 1971 book The Mechanics of Independence, ANR Robinson wrote that: ‘As financial rewards are lower in the Read more
Want to share your thoughts with Wired868? Email us at editor@wired868.com.
Please keep your letter between 300 to 600 words and be sure to read it over first for typos and punctuation.
We don’t publish anonymously unless there is a good reason, such as an obvious threat of harassment or job loss.
